Conference season is here, and this time EPoCH attended their first in person meeting in 2 years (due to Covid-19 restrictions). I attended a wonderful symposium arranged by the Centre for Fertility and Health (CeFH) in Oslo, Norway, and was also invited to visit CeFH afterwards to give a presentation about all of EPoCH’s work so far.
Beautiful Oslo
The symposium focused on the underlying causes and consequences of changing fertility and family patterns using national data. Day 1 started with quick-fire presentations from current PhD students and postdocs for ongoing and planned research. It was great to hear the range of work happening and was obviously exciting for us to hear that research being undertaken also included paternal data! Presentations were given on the influence of unemployment from paternal plant closures on children’s health care usage, as well as how grandfathers involvement in a child’s upbringing could impact offspring health. The seminar’s final day discussed amongst other things current research being undertaken for intergenerational effects as well as future plans to research Covid-19 and pregnancy within the CeFH.
This trip was exciting for many reasons. Not only as it was the first physical trip out of Bristol for EPoCH in a long time, it also gave me the opportunity to meet with collaborators from the Norwegian Mother, Father and Child Cohort Study (MoBA) whom we’ve been working with virtually since the start of the project. Not to mention the beautiful landscape of Oslo, which the CeFH chose to showcase with an organised dinner venue of Ekebergrestauranten overlooking the harbour.
The view from dinner at Ekebergrestauranten
EPoCH had lots of travel plans at different research institutions for this project which unfortunately we have so far been unable to conduct. But with travel restrictions lessening we should hopefully have some more trips lined up to tell you about!
Back in June 2020, Kayleigh had planned to attend two exciting back-to-back conferences in Boston, USA (Society for Epidemiologic Research/ Society for Pediatric and Perinatal Epidemiologic Research). However, as the Covid-19 pandemic progressed, it became clear that an in-person conference would no longer be on the cards and instead both conferences were moved to be held online in December.
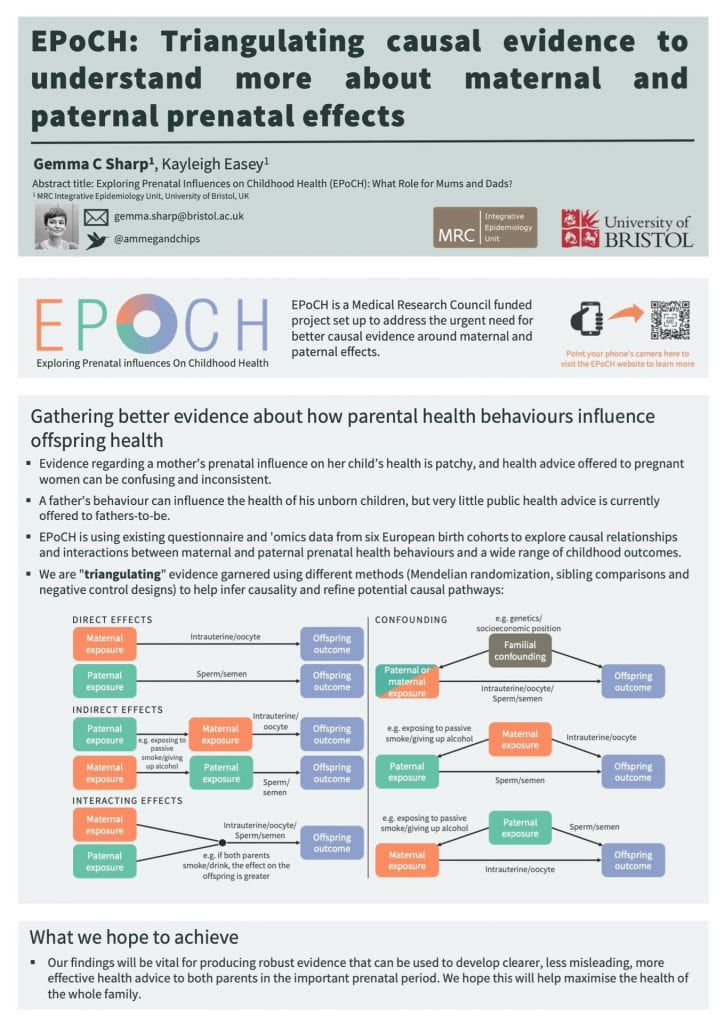
Going to a virtual conference was admittedly a different experience to in-person, and the -7 hour time difference of live talks being broadcast at first felt challenging. But luckily all sessions were recorded so we could catch up on any we missed! Kayleigh presented an online poster (shown below) which details our EPoCH study.
This year we were excited to see more talks that focused on paternal exposures around conception and their influence on offspring health. In particular paternal exposure to plastics seemed to feature heavily…this isn’t an exposure that we were including in EPoCH ourselves, but it was definitely thought provoking. We were also glad to hear many talks focusing on selection bias within pediatric epidemiology, and the effects this can have on the data we use. This is a topic that we are currently writing a paper on, and hope to share with you later this year!
The next SER/SPER conference is planned to take place (optimistically) in-person during the summer of 2021 in San Diego, and we hope that we can still take part even if from the comfort of our homes again whilst watching online…
This week we are happy to say EPoCH hosted its first Research Advisory Panel meeting. As we were no longer able to host this event in person due to Covid-19, we embraced the online video apps to help us make sure this event could still take place. And we are pleased to say that the meeting was a great success, with members from varying geographical locations able to attend…and all from the comfort of their own homes.
So why have we created the advisory panel? We wanted to make sure that any findings we may have from the EPoCH study are able to reach people in the right way, and that we don’t end up accidentally adding to the confusion around health advice during pregnancy. This is why the Research Advisory Panel was assembled! Within this panel we currently have members from varying backgrounds who have all expressed an interest in taking part. Each panel member is sent an update on our progress from the project every 3 months and invited to a ‘face to face’ or more likely atm a “computer screen to screen’ meeting every six months, to discuss what we’ve been doing.
This week’s first meeting gave us all a chance to meet each other, as well as provide the panel with updates on our progress in the project so far. Gemma and I were joined by Lindsey Pike who brilliantly chaired the meeting, as we ventured into the online world of group video calls.
Alongside Gemma, Lindsey and myself, attendees at our first meeting were:
Kirsty Budds (Leeds Beckett)
Rebecca Goldman (Fatherhood Institute)
Jon Symonds (University of Bristol)
Line Hjort (Rigshospitalet, Copenhagen)
Carina Venter (University of Colorado Denver)
Sangeetha Shyam (International Medical University Malaysia)
Rebecca Blaylock (BPAS)
We are very thankful to all current members for such an enjoyable meeting and look forward to our next catch up in six months’ time!
At the start of January, Gemma attended a workshop in London held by the Parent Infant Foundation as part of their 1001 Critical Days movement.
The movement is an alliance of charities, parliamentarians, practitioners and academics that campaigns to ensure that all babies have the best possible chance in life.
The 1001 critical days are the period between conception and a child’s second birthday. The Movement is based on evidence suggesting that, during this time of rapid growth, relationships with parents and other caregivers are incredibly important. What happens during this time lays the foundations for future wellbeing development.
Together, the Conception to Age Two All-Party Parliamentary Group and the wider 1001 Critical Days Movement raise awareness of the importance of this life stage, particularly amongst MPs who can affect change.
The aim of the workshop was to co-create the 1001 Critical Day’s future vision, strategy and plans to enable them to achieve more for babies and their families.
Gemma was there to learn more about the role of the movement and gain insight into how a cross-party parliamentary group works. She also tried to emphasise the importance of not focusing solely on mothers and making individual women feel guilty, but rather looking at paternal factors and wider societal contexts as well. Reassuringly, other workshop attendees were very much on board with this and had similar comments from their own perspectives.
In EPoCH, we will continue to follow the work of the 1001 critical days movement and contribute where we can. A greater appreciation of the importance of the pregnancy and early postnatal period amongst policy makers will help ensure that any important findings coming out of EPoCH are effectively translated into policy around pregnancy advice.
Back in October 2019, Kayleigh and Gemma attended the Developmental Origins of Health and Disease (DOHaD) conference in Melbourne, Australia.
Kayleigh presenting her maternal alcohol pheWAS paper
Kayleigh gave a talk on a project she completed as part of her PhD. Conference attendees were very interested in her pheWAS (phenome-wise association study) of maternal alcohol consumption during pregnancy. Kayleigh is preparing a paper describing the results at the moment, and we will no doubt write a blog summarising what she found when it is published.
Gemma presenting her talk entitled “You are (not really) what your mother ate”
Gemma was very busy at the conference: presenting at two pre-conference workshops, giving one invited talk, giving an interview to a South African podcast and presenting not one but three posters! All her posters are shown below, and she hopes to upload a video of her talk soon.
Back in May, Gemma took part in Creative Reactions, an initiative that pairs scientists with artists to create artwork based on their academic research.
Gemma was paired with Olga Trevisan, an artist based in Venice, Italy. They had conversations over Skype where they spoke about their work and formed some initial ideas about how they could combine their interests in a new way while remaining coherent to their own practices. Reflecting on the collaboration, Olga said, “I love how curious you can be of a subject you haven’t considered before. I believe collaboration helps to open your own mind.”
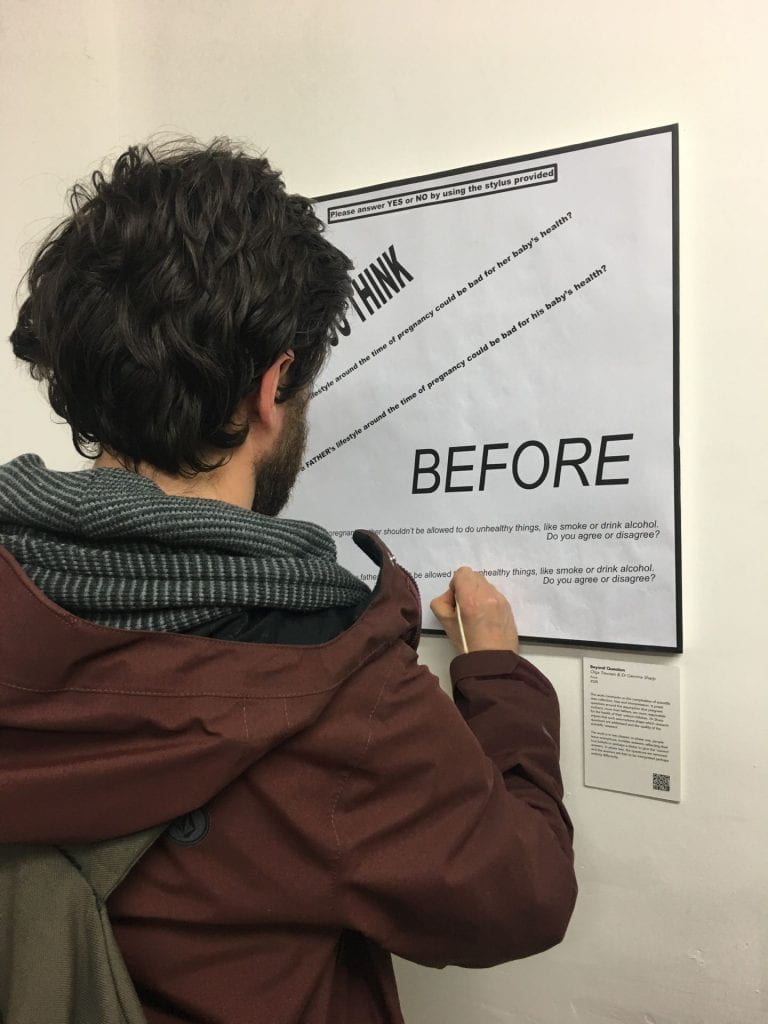
Based on some of the work around EPoCH, Olga created a piece called Beyond Question, which comments on the complexities of scientific data collection, bias and interpretation.
It poses questions around the pervasive assumption that pregnant women are more responsible for the (ill) health of their unborn children than their male partners are. Gemma and colleagues have argued that such assumptions drive the research agenda and the public perception of parental roles, by shaping which research questions get asked, which data are collected, and the quality of the scientific ‘answer’.
Photo credit: Olga Trevisan
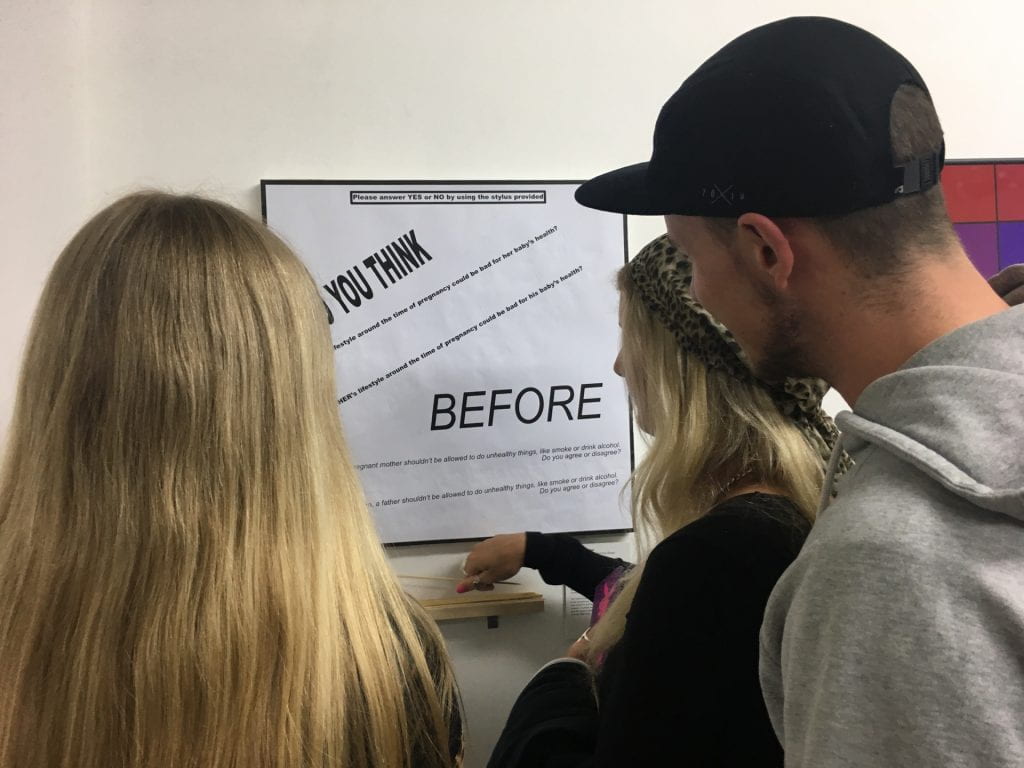
Beyond Question was presented in two phases at two separate exhibitions: during the first phase, people were invited to answer questions with a simple Yes or No using a stylus; leaving no marks but only invisible, anonymous traces on the surface below. Answers will reflect the real assumptions, beliefs and attitudes of the respondent, but perhaps also, despite anonymity, their eagerness to ‘please’ the questioners, to give the ‘right’ answer, and to mask their true responses to paint themselves in the ‘best’ light.
In the second phase, the questions were removed and the answer traces were left alone to carry their own meaning; free to be combined with the attitudes, beliefs and assumptions of the viewer and to be interpreted and judged in perhaps an entirely different way.
Photo credit: Olga Trevisan
The questions posed were: “Do you think a mother’s lifestyle around the time of pregnancy could be bad for her baby’s health?”; “Do you think a father’s lifestyle around the time of pregnancy could be bad for his baby’s health?”; “Before her baby is born, a pregnant mother shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”; “Before his baby is born, a father shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”
We want to make sure that EPoCH research findings reach the right people in the right way and we don’t accidentally end up adding to the confusion around health advice during pregnancy.
Therefore, we are setting up a Research Advisory Panel of researchers, policy makers and people with real life experience of giving and receiving pregnancy advice.
What will panel members do?
Panel members will give us feedback on our plans, and tell us how they think we can best communicate our findings in the most appropriate, effective way. In return, we will keep panel members up to date on our findings, and they will be invited to the academic and/or public events that we organise. It’s a great opportunity to get involved with some exciting research from the University of Bristol.
When people sign up to the panel, they will answer a few short questions to get their opinions about EPoCH. We’ll then create a summary of everyone’s responses, which we’ll share with the other panel members. We’ll also explain how we’ve taken their responses on board and how this has affected our future plans.
After this initial survey, we’ll be in touch every time we have some exciting news to share (but we promise not to spam people!). We’ll also send mini reports every six months or so and ask for panel members’ comments and ideas. Occasionally, if panel members agree it would be useful, we might set up teleconferences or face-to-face meetings to discuss further.
How can people join the panel?
If you’re interested in joining the panel, please fill out this short survey.
I am excited to say that I have just started working as a Senior Research Associate on the EPoCH study! I have recently completed my PhD at the University of Bristol which investigated the association between exposures in pregnancy (mainly prenatal alcohol use) and offspring mental health outcomes in late adolescence. I am lucky enough to have found a project which allows me to continue working within this area, and even better to be able to explore different exposures and outcomes of interest.
About me…
Before I started a PhD here in Bristol my background was predominately in mental health research. After completing my undergraduate degree in Psychology, I gained experience within the NHS as an Assistant Clinical Psychologist. This allowed me initially to conduct clinical research within mental health departments across Devon, and eventually led me to train as a mental health therapist. I became further interested in the causal nature of mental health problems and how we may be able to improve outcomes, which ultimately led me back into research. I then completed a MSc in Health Psychology at the University of Bath, and afterwards began working as a Research Associate within the Tobacco and Alcohol Research Group (TARG) at the University of Bristol. Having developed an interest in how different health behaviours can influence mental health outcomes, this led to the start of my PhD and a shift into learning and utilizing epidemiological methods to investigate the true causal effect.
Fast forward four years, and here I am in the EPoCH study with Gemma, ready to investigate multiple exposures during pregnancy (both maternal and paternal) on a wide range of offspring outcomes using various birth cohorts around the world. Get ready for updates from me here in the EPoCH blog over the next three years on the work we’re doing…
A novel thing about EPoCH is that we’re not just focusing on maternal influences on offspring health, we’re looking at paternal influences as well.
One of the reasons that most other studies have focused on maternal factors is that it’s perhaps easier to see how mothers might have an effect on their child’s health. After all, the fetus develops inside the mother’s body for nine months and often continues to be supported by her breastmilk throughout infancy. However, in a new paper from me and Debbie Lawlor published in the journal Diabetologia, we explain that there are lots of ways that fathers might affect their child’s health as well, and appreciating this could have really important implications. The paper focuses on obesity and type two diabetes, but the points we make are relevant to other health traits and diseases as well.
How could fathers influence the health of their children?
These are the main mechanisms we discuss in the paper:
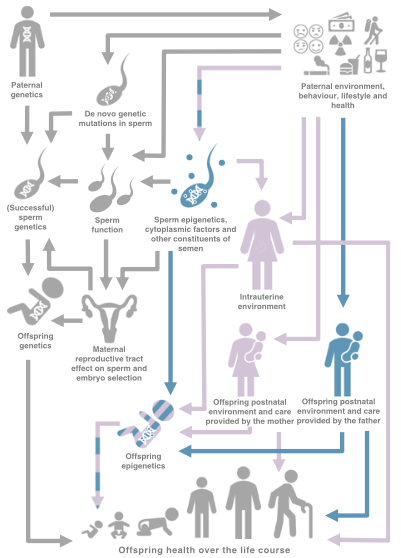
Through paternal DNA. A father contributes around half of their child’s DNA, so it’s easy to see how a father’s genetic risk of disease can be transmitted across generations. Furthermore, a father’s environment and behaviour (e.g. smoking) could damage sperm and cause genetic mutations in sperm DNA, which could be passed on to his child.
Through “epigenetic” effects in sperm. The term “epigenetics” refers to molecular changes that affect how the body interprets DNA, without any changes occurring to the DNA sequence itself. Some evidence suggests that a father’s environment and lifestyle can cause epigenetic changes in his sperm, that could then be passed on to his child. These epigenetic changes might influence the child’s health and risk of disease.
Through a paternal influence on the child after birth. There are lots of ways a father can influence their child’s environment, which can in turn affect the child’s health. This includes things like how often the father looks after the child, his parenting style, his activity levels, what he feeds the child, etc.
Through a father’s influence on the child’s mother. During pregnancy, a father can influence a mother’s environment and physiology through things like causing her stress or giving her emotional support. This might have an effect on the fetus developing in her womb. After the birth of the child, a father might influence the type and level of child care a mother is able to provide, which could have a knock-on effect on child health.
There are lots of ways in which fathers might influence the health of their offspring. This figure was originally published in our paper in Diabetologia (rdcu.be/bPCBa).
What does this mean for public health, clinical practice and society?
Appreciating the role of fathers means that fathers could be given advice and support to help improve offspring health, and their own. Currently hardly any advice is offered to fathers-to-be, so this would be an important step forward. Understanding the role of fathers would also help challenge assumptions that mothers are the most important causal factor shaping their children’s health. This could help lessen the blame sometimes placed on mothers for the ill health of the next generation.
What’s the current evidence like?
In the paper, we reviewed all the current literature we could find on paternal effects on offspring risk of obesity and type 2 diabetes. We found that, although there have been about 116 studies, this is far less than the number of studies looking at maternal effects. Also, a lot of these studies just show correlations between paternal factors and offspring health (and correlation does not equal causation!).
What is needed now is a concerted effort to find out how much paternal factors actually causally affect offspring health. This is exactly what EPoCH is trying to do, so watch this space!
Mendelian randomization is one of the techniques EPoCH uses to understand whether parents’ lifestyles in the prenatal period causally affect the health of their children.
The technique (which cool kids call ‘MR’) is based on the idea that genetics can tell us about non-genetic factors and their effects on health and disease.
Many of the people I work with at the University of Bristol (most notably the director of the MRC Integrative Epidemiology Unit, George Davey Smith) have championed MR, and over the past decade there has been a huge increase in the number of published MR studies.
To be honest, I struggled with understanding MR when I started working at the University of Bristol. At one early department meeting I asked whether there was “a course or something on MR for Dummies?” Thus charming my new colleagues with my cutesy self-deprecating wit.
And I know it’s not just me, because I have tried to explain MR to multiple confused faces belonging to students, academics, clinicians, members of the public, and, most bemused of all, my friends and family (“WHY is she telling us this?”).
But now that I’m the principal investigator on a grant that includes MR, I want to be able to explain it in a way that other people understand, so here goes…
MR helps us tell the difference between correlation and causation
MR uses the chance (or “random”) distribution of genes in a population to tell us about whether certain non-genetic characteristics or behaviours cause other characteristics or disease. I’ve written more about why distinguishing correlation from causation is important here.
Genetic data as a “proxy”
MR uses genetic information as a “proxy” for non-genetic information. For example, people with a certain variant of the ALDH2 gene (let’s call it variant 1) are much more likely to drink alcohol than people with another variant (let’s call it variant 2). So if we want to study the effects of parents’ alcohol consumption on offspring birth weight, we can compare the average birth weight in babies of parents with variant 1 to the average in babies of parents with variant 2.
This can give us a better idea of causation than if we just tried to study this by asking parents how much they drink (i.e. if we didn’t use their genetic information).
That’s because genetic information is randomised at conception, so the chance of someone getting variant 1 or variant 2 is random and not affected by any confounding factors. On the other hand, how much alcohol parents drink will be heavily influenced by confounding factors such as how much money they have, where they live, their religion, etc.
Parents might also forget how much alcohol they have consumed, or under-report it, which would introduce reporting bias. Genetic information is measured objectively and therefore not affected by this type of bias.
Also, because genetic variants are assigned at conception and then can’t be changed, there’s no chance that the outcome (birth weight) can influence the exposure (parents’ alcohol intake), so reverse causation is not an issue in MR either.
(…reverse causation is unlikely to be much of an issue in EPoCH anyway, because we know that the exposure (e.g. drinking alcohol during pregnancy) always comes before the outcome (e.g. weight at birth) in this study).
How EPoCH will use MR
In EPoCH, we’ll use MR to study the causal effects of maternal and paternal health behaviours on childhood health. Although there is lots of observational evidence suggesting that parental (particularly maternal) factors are associated with the health of their children, very few studies have looked at whether these associations are causal.
The assumptions of MR
MR can be a really useful tool for “causal inference”, but there are many things to consider before drawing conclusions. In particular, we need to check that the following main “assumptions of MR” are being met.
The relevance assumption
To be suitable for MR, a genetic variant should be very strongly associated with the exposure being studied. So in our example, having variant 1 of ALDH2 must be very strongly associated with drinking more alcohol.
The independence assumption
The genetic variant must not be affected by any of the other factors that affect the outcome, i.e. the association between the genetic variant and the outcome must not be confounded. So smoking (etc) shouldn’t affect the chances of having ALDH2 variant 1 or 2.
The exclusion restriction assumption
The effect of the genetic variant on the outcome should not act via any pathway that doesn’t involve the exposure. So having ALDH2 variant 1 should not affect birth weight through any pathway that doesn’t involve an effect on drinking alcohol. E.g. ALDH2 variant 1 should not affect how much a person smokes, because this might then have a causal effect on offspring birth weight independently of any effect of alcohol consumption.
How can we be sure MR is giving us the right answer?
Neil Davies, Michael Holmes and George Davey Smith have written an excellent introduction to MR that outlines how we can check that the assumptions of MR are being met. We’ll be doing all we can in EPoCH to check these assumptions. However, even with multiple checks, it will be difficult to tell that an answer is “right” using MR alone.
That’s why we’re combining MR with other causal inference techniques, such as sibling comparisons and negative control designs, to “triangulate” the evidence. If all these different strands of evidence point towards the same answer, then that will strengthen our confidence that the answer is correct.
A two minute explainer
Well that was my attempt to explain MR, but if you’re still confused, George manages to explain it much more eloquently in just two minutes in the following animation…
(I probably should’ve just posted this and saved everyone’s time… soz).